
BeamReaders Blog
>
How to Get a Better CBCT Report: Scan Quality, Submission, and When to Refer to an OMR
This article is based on a webinar led by Dr. Srinitha Singanamala and Dr. Anne Dorsey, Oral and Maxillofacial Radiologists at BeamReaders. In the session, they walked through how to turn your CBCT submission into the most useful report possible, from the moment you decide to refer to the moment the report lands back in your inbox. The basis is simple: great information in, great report out.
To be clear, every volume gets a comprehensive, documented read regardless of what you send. That is the standard of care, and it does not change. What good information changes is how quickly the report comes back, how tightly it answers your clinical question, and how often the radiologist has to pause and reach out for something they could have had up front – which take valuable time for you to follow up.
You are the clinical expert for the patient in the chair. The radiologist is the imaging expert with a trained eye on every slice of the volume. The recap below is about creating a great handoff.
Before any of the submission mechanics and handoffs occur, it’s vital to understand that the standard of care requires a written, documented review on every CBCT you capture. Dr. Singanamala put it plainly: “You would not place a filling without a note, so do not capture a volume without a documented interpretation.” Whether you write it or an oral and maxillofacial radiologist does, it needs to exist. It supports patient care, it documents that the volume was reviewed, and it supports your defensibility.
The Traffic Light Protocol is the framework for deciding who writes that report.
A key red light qualified is related to uncertainty. As Dr. Dorsey put it, recognizing uncertainty is not a weakness. Even experienced oral radiologists consult each other, and even after four decades in the field, BeamReaders founder Dr. David Hatcher always likes to say, “I think I've seen it all until I open that next volume."
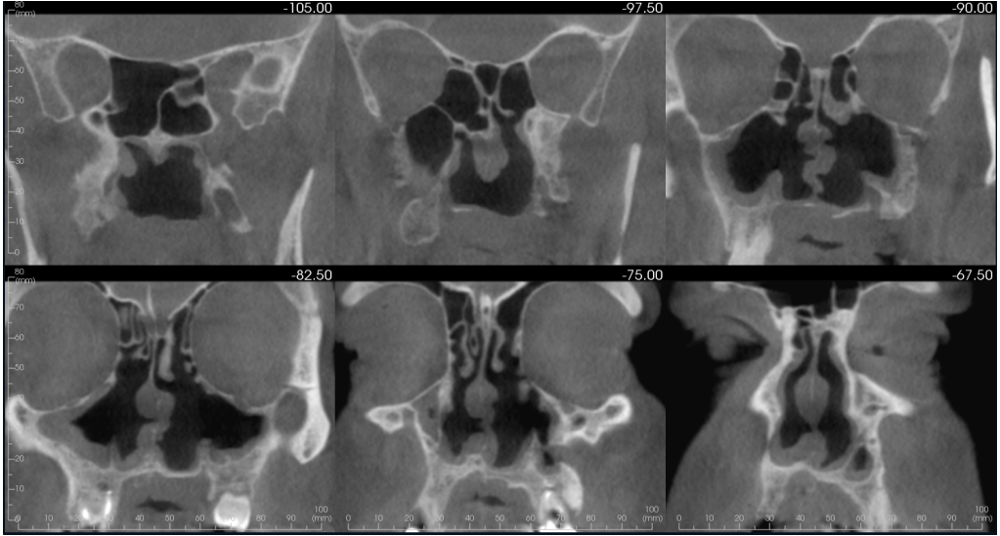
A large field of view tends to land in red on its own. In the webinar, Dr. Singanamala shared a case submitted to her with no clinical notes and no history. On full-volume review she identified extensive destructive sinonasal changes and noted a differential of granulomatosis with polyangiitis, which was later confirmed on pathology. The case needed an expedited ENT referral. The full read happened despite the absence of any context, which is the point, and the field of view alone was reason enough to refer.
The Traffic Light Protocol is a free download. If you want the framework to bring to your team, you can grab the eBook here.
The report can only be as clear as the volume, and there are a few key takeaways from the session to help you and your imaging technicians protect image quality:
This is where small changes on your side make the biggest difference for oral radiologists. The most common issues seen relate to incomplete uploads, mismatched patient details, poor image quality, missing prior records, and unclear urgency. Each one tends to cost time rather than thoroughness.
A few practices that prevent the back-and-forth:
On that last point, Dr. Dorsey described a referral that arrived marked only "please evaluate," with no site and no clinical question. Because the volume gets a full read either way, she began her systematic review while reaching out through RadChat.
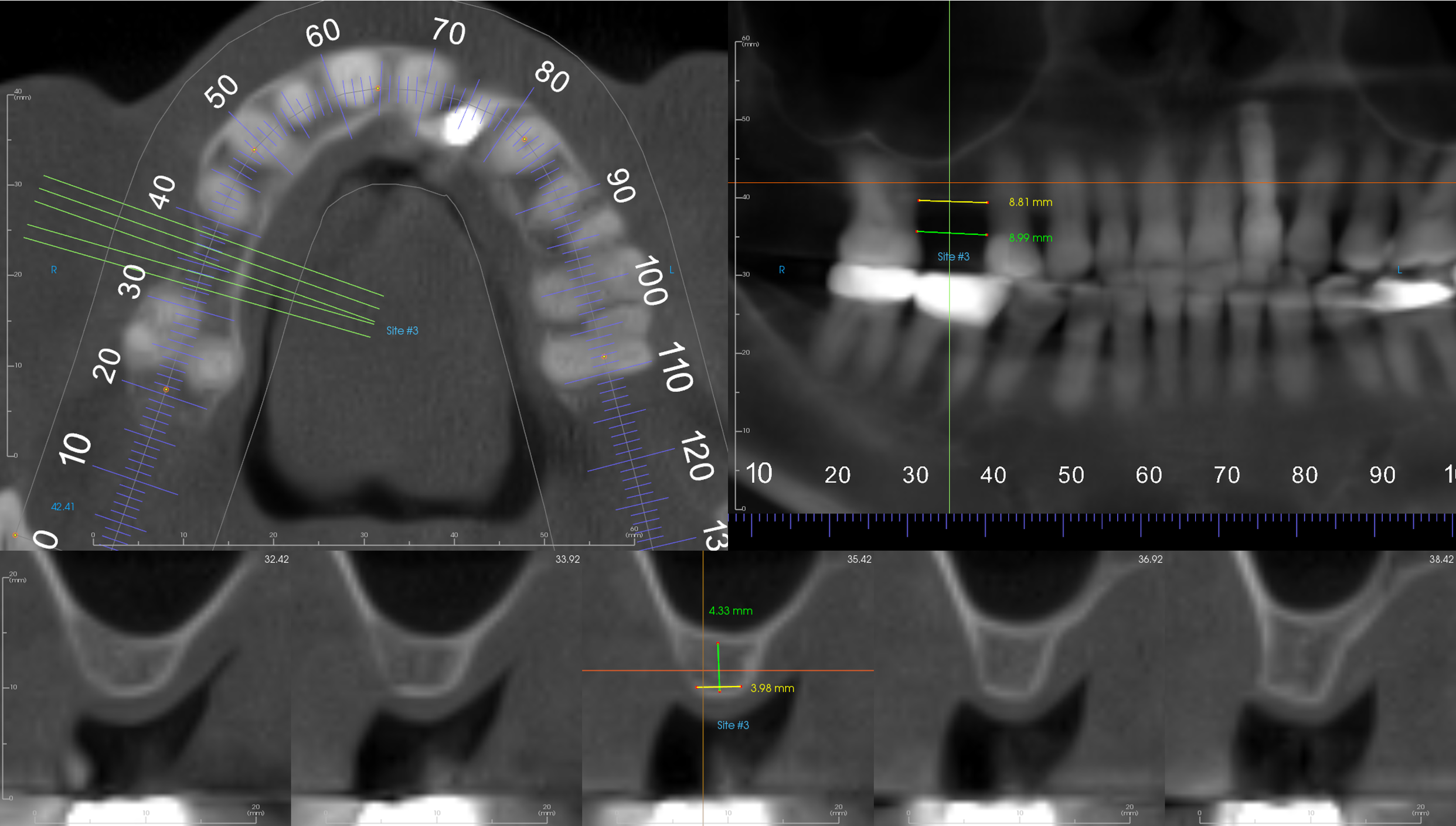
She worked through the airway, the nasal cavity, and the TMJ, the things this long-standing practice usually cares about. Days later the practice clarified what they actually wanted: an implant evaluation at site number three. That is a focused deliverable, including a dedicated implant image, that the report does not generate unless it is requested. The full review happened regardless. What the missing detail cost was several days and a round of back-and-forth.
Most cases run on a three to five business day turnaround. When a patient needs faster, there are rush options. In another example, a practice sent a large field of view study for a patient with recent-onset pain, crepitus, joint popping, and referred ear symptoms including tinnitus and vertigo. It was a model submission: clinical relevance, the treatment pathway, and a request for an expedited read. The referring doctor even called to flag it before the patient left the chair.
On review, Dr. Dorsey identified an ill-defined hypodense lesion involving a large portion of the temporal bone, a finding that raises concern for either inflammation or malignancy. The patient was referred urgently to an ENT for advanced imaging, and because the urgency was flagged up front, the process moved quickly. It was determined to be inflammation, and the patient was brought out of pain.
RadChat is direct communication between you and your radiologist, built into the patient's profile and never visible to the patient. It is the right place for a clinical concern you do not want on the report itself, or a note that a patient struggled to hold still.
When the radiologists were asked what helps most, the answer came down to three things:
Even a sentence or two about symptoms, duration, or prior treatment helps. So do prior reports, periapicals, a pan for comparison, clinical photographs, pathology results, and relevant history. Context lets the radiologist connect what they see to the question you are asking.
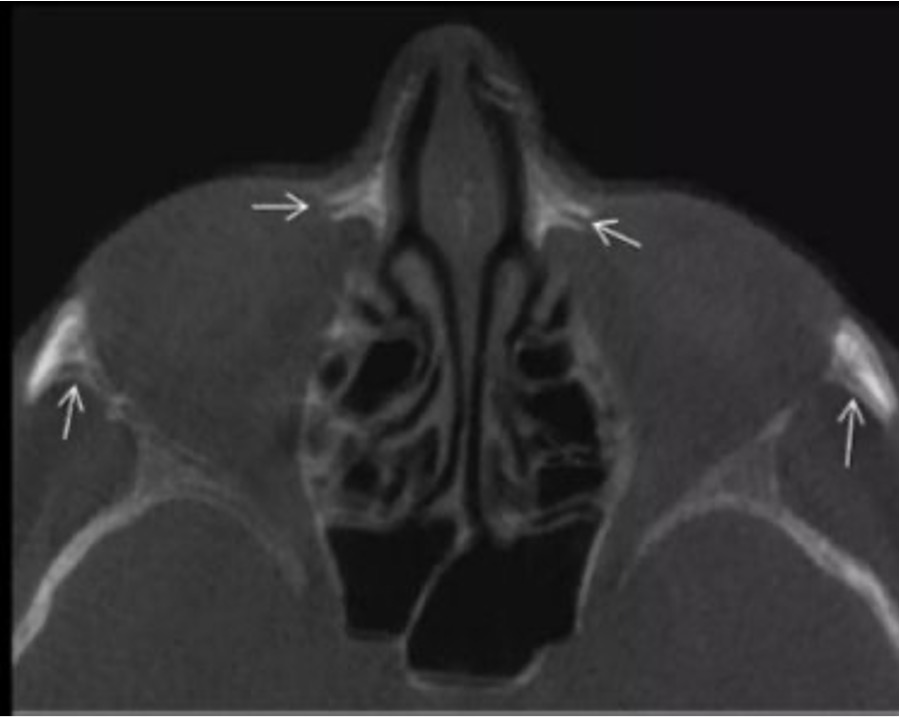
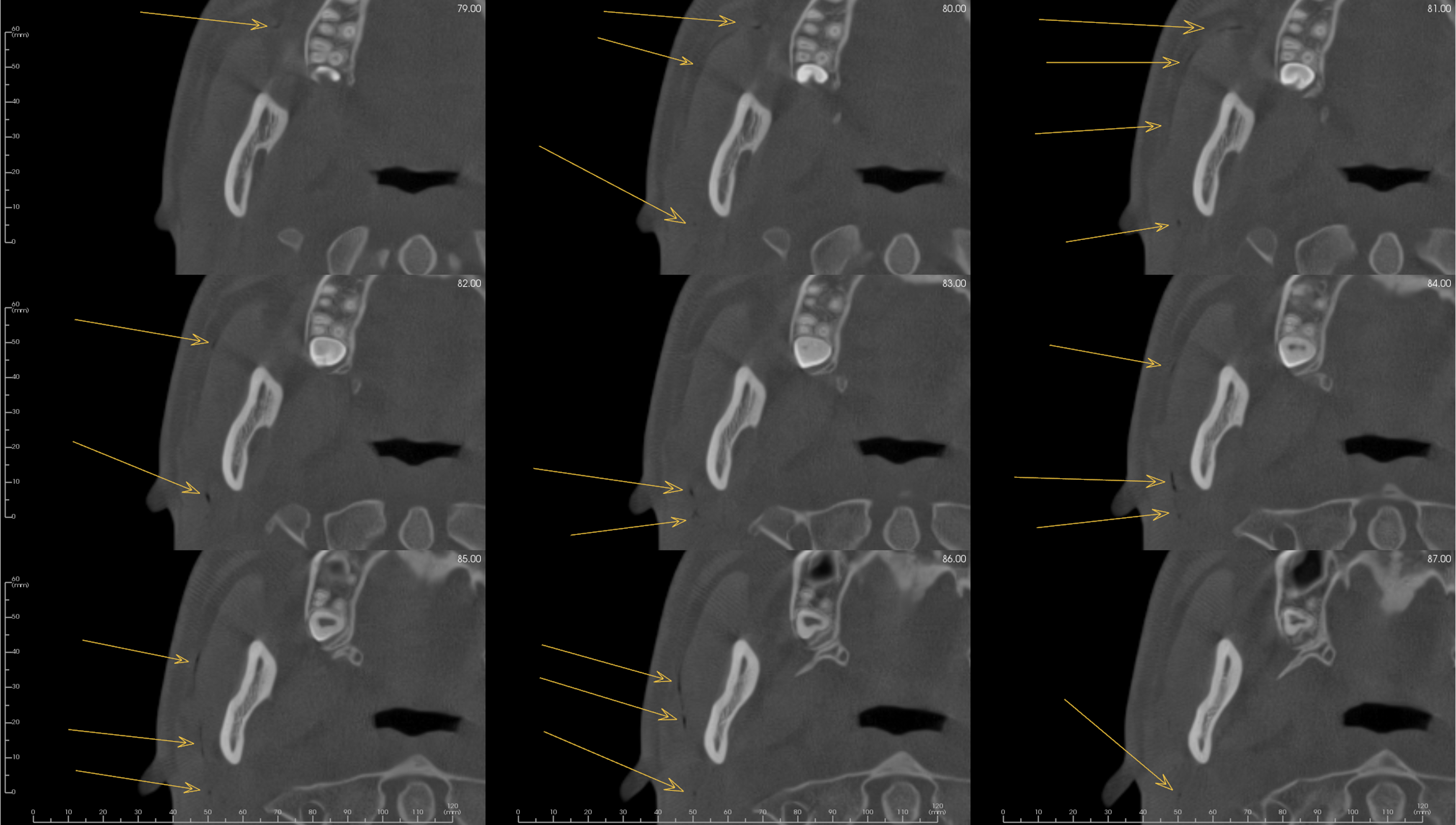
A third case from the session shows what that makes possible. A practice submitted a large field of view scan with a clear airway question, since the patient was reporting airway concerns. During the systematic review, Dr. Dorsey identified a linear hypodensity tracing the parotid duct.
The most likely explanation was introduced ductal emphysema, familiar in everyday dentistry, though air in that location can also represent infection or a pneumoparotid. The practice was not aware of it, and the patient was not yet symptomatic. The finding shifted the care plan, and the patient was managed early. The airway question was answered as well: a radiologically limited airway with nasal mucosal thickening, which led to an ENT and allergist referral.
While the volume always gets a comprehensive read by our oral and maxillofacial radiologists, better scans, better input, and better communication makes a difference. What you provide at submission determines how fast it comes back, how closely it answers your question, and how much time both sides save.
Radiologists are not a dental report generation service sitting at a distance. They are part of your care team, and when they have what they need, they can be a far more useful partner in your patients’ care.
If you want the full session, including both example walkthroughs, watch the recording here.
And if you do not yet have a referral protocol in place, download the Traffic Light Protocol and bring it to your next team meeting.
Questions about a submission, or want to work with a specific radiologist on a case? Reach the team at education@beamreaders.com.



